A week after the dedication of the new Mountrail Bethel Home nursing home section, there was another gathering on Wednesday, March 11, at the Mountrail Bethel Home. This time, those gathering were there to say goodbye. This was a time for families to return, remember, and give thanks. It was one last visit to the original nursing home before it is taken down, including a prayer of blessing and an opportunity to visit loved ones’ rooms.
The hallways already show the beginning of the work to take down the north and south wings of the old nursing home. It was quiet in the gathering space, a place that was used by residents for many of their activities throughout the day.
Pastor Erin Tormanen offered his thanks for these spaces that held a special place in the hearts of those attending. This day was a time to remember those who had made the rooms their home and where they lost many of them. He says this is true in nursing homes, where those living there were cared for in the last chapters of their lives.
He asked that the memories continue to be a blessing. As they were taking one last walk through the spaces, he encouraged those attending to remember the faces and let the memories come back as a precious gift from God. He encouraged them to let the memories flood in and fill them with the love and life they shared.
Angels were left on the ledges in the old nursing home with those attending encouraged to take those home with them. They were given a time to wander and see these spaces in whatever manner they chose before leaving.
Crews are beginning the work in the north and south wings as they prepare for the next phases of construction that will lead to the hospital renovations. It will start with the removal of the old nursing home wings to create a new entrance and parking area.
There will be a gift shop and a new waiting room. Construction down the current south wing of the nursing home will include adding an out-patient infusion suite, pharmacy suite and an MRI suite.
Purchasing will be moving from the basement to the upper level. The downstairs area will be renovated to accommodate a new specialty clinic that will allow the facility to bring in more specialists. It will also include a minor procedure room.
The final phase of construction will be adding seven new apartments to Rosen Place. The assisted living facility always has an extensive waiting list, showing the need for the new apartments. These will all be single apartments based on the footprint space available.
The entire project cost is estimated at $47 million, with $29 million of that for the new nursing home. The Mountrail County Commissioners committed $25 million over two years for the nursing home portion of the project. Other donors and fundraising efforts have left the entire project with $5 million left to raise. The Foundation continues to accept donations from the public including the ability to donate on their website: www.mountrailcountyhealthfoundation.org/how-you-canhelp.
Wednesday, March 4, was a big day at the Mountrail Bethel Home in Stanley as the new nursing home was opened to the public for the first time with a dedication and open house in the afternoon.
The day began earlier for the residents of Mountrail Bethel Home as they got their first look at what will be their new home in the morning. Residents were able to participate in a ribbon-cutting ceremony that included a prayer of dedication with activities director Chuck Repnow.
Following the ribbon cutting, they were able to tour the new facility and find their new rooms. Faces lit up as they were given their tours of all of the new spaces before going back to the older wings of the nursing home for now. Residents were expected to begin moving into their new rooms on Monday, March 9.
The new rooms are larger and more modern. There is a new family room for private events and a new outdoor patio with fire pits and grill. The facility also added a new beauty and nail salon for residents.
The dedication ceremony was one of thanks, opening with Administrator Steph Everett welcoming everyone to this new nursing home which has been decades in the making. She thanked board members who have made this positive decision over the years and construction company McGough for their beautiful work. She said the generosity of donors, including the Mountrail County Commissioners, have made this possible. She also thanked the staff for their “all hands on deck” work to get ready for this day. She looks forward to the amazing resident and patient care that will come from the entire project.
Dr. Mark Longmuir said this is a new chapter in the lives of the residents. It is a celebration of the commitment of all in the community. He thanked family members for trusting the facility to care for their loved ones.
While this is a new journey for all, the new facility is the representation of decades of planning and a shared belief that everyone deserves the very best.
He thanked all those who have put in so much time and effort getting to this point, including McGough and their contractors, CEO Steph Everett for her work put into the planning and details, Jim Clark for the decades of work preparing for this project, and the maintenance staff and housekeeping staff for the work preparing for this day.
To the residents, he said this opens a new chapter of joy, peace and love, ending with “welcome home”.
Board member Heath Hetzel said that projects like this take change. The community will continue to see that change when the north and south wings of the old nursing home begin coming down.
He also pointed to the chapel at Bethel Home, which is amazing. When the north wing comes down, that chapel and its beauty will become a focal point.
He also expressed how excited they are to have a new home for the residents and gave all glory to God for the process.
Current MBH board chairman Ryan Gjellstad gave his thanks to all of the staff and commended them for the work to take care of everything, saying he has all the confidence in the world in the future of the facility.
Former board president Bob Grant said that over twenty years ago, while he was on the board, they discussed what they could do to help the residents but they faced the space struggles. They looked at whether they should remodel, fix or build again, all the while wondering what it would take.
Looking at the way the facility is now a campus with the nursing home, hospital, clinic and assisted living, he commends those who followed after them for following through. He, too, looks forward to seeing the chapel as a front focal point for the facility. He ended by saying that he is proud of all they have done, building for the future and adapting to the changes.
Former board president George Olson remembered the time in the 1950s when the homes in rural communities were filled with older, retired people. They were faced with the challenge of what to do to help them. It was these people who formed the committee and created MBH and he is thankful for that. He said this new facility is a place where people can come and be blessed again. He expressed his gratitude to the community, the generations before us, and those to come.
Pastor Erin Tormanen reflected on the official groundbreaking on July 17, 2024, with the goal of MBH to create an environment that works to satisfy the physical, emotional and spiritual needs for the residents and their families.
While the physical facility is now here, it is more than a building. It takes love, personal and intimate care for those residents. The command to love and take care of our neighbors is woven through God’s creation and scripture. He offered praise to God for all of the efforts to bring forth this facility, making it a glorious reality to serve those precious and beautiful souls that will come in and fill the rooms. He ended with a prayer of dedication for this new facility.
Following the official ceremonies, those attending were treated to an amazing charcuterie spread that filled the nurses’ station. Those attending were also allowed to tour the facility, checking out all of the amazing new spaces and rooms.
Groundbreaking on the new nursing home was held on July 17, 2024. This first phase of construction is the new 36 bed nursing home, including ten basic care rooms. This is the same number of beds as the former nursing home.
With that work now complete, construction will move to the hospital renovations. Those will start with the removal of the old nursing home wings to create a new entrance and parking area. The public is invited to join the facility again as they host a farewell to the original Mountrail Bethel Home on Wednesday, March 11 at 12:00 noon. This will be a time for families to return, remember and give thanks. It will be one last visit to the original nursing home before it is taken down, including a prayer of blessing and opportunity to visit loved ones’ rooms.
There will be a gift shop and a new waiting room. Construction down the current south wing of the nursing home will include adding an out-patient infusion suite, pharmacy suite and an MRI suite.
Purchasing will be moving from the basement to the upper level. The downstairs area will be renovated to accommodate a new specialty clinic that will allow the facility to bring in more specialists. It will also include a minor procedure room.
The final phase of construction will be adding seven new apartments to Rosen Place. The assisted living facility currently always has an extensive waiting list, showing the need for the new apartments. These will all be single apartments based on the footprint space available.
The entire project cost is estimated at $47 million, with $29 million of that for the new nursing home. The Mountrail County Commissioners committed $25 million over two years for the nursing home portion of the project. Other donors and fundraising efforts have left the entire project with $5 million left to raise. The Foundation continues to accept donations from the public including the ability to donate on their website:www.mountrailcountyhealthfoundation.org/how-you-canhelp.
Jill Schramm/MDN Construction workers with McGough raise wall supports inside what will be a new nursing home at Mountrail County Health Center on Feb. 24.
STANLEY – Mountrail County Health Center in Stanley has launched a three-year, $53 million construction project designed to enhance care for its community and particularly for its long-term care residents.
Currently, the contractor, McGough, has construction underway on a new 46-bed skilled and basic care facility to replace the existing Mountrail Bethel Home, with completion expected in March 2026.
“We’ve talked about this project forever, so I’m excited to have it come to fruition,” said Stephanie Everett, administrator and foundation director for MCHC. “The residents deserve a nice home.”
The 60 year old nursing home building is showing its age, she said. Pipes are crumbling. Bathrooms are too small to accommodate lifts and barely fit wheelchairs.
The new nursing home will have 36 skilled care beds and 10 basic care beds, as does the existing facility. Everett said maintaining the number of beds is important with the continued aging of the Baby Boom generation.
A couple of construction workers with McGough secure exterior covering on the side of a section of a new long-term care facility in Stanley Feb. 24.
Visitors entering the new nursing home will be greeted by the nursing station, located near a large, open area with tall ceilings and large windows.
“We want to have events, but sometimes we have to take it off campus because we just don’t have the space. So, we’ll be able to now have this great space to have our health fairs and all kinds of different events that we want to do,” Everett said.
The new nursing home will offer mostly private rooms, with more spacious rooms and full-sized beds. There will be two double rooms available for skilled or basic care per state requirements.
Green spaces and patios will be located around the facility, with a patio area with a firepit just outside the facility’s family room. A new beauty and nail salon will replace the current salon space.
North Dakota law allows counties to donate to local medical centers for new construction. The Mountrail County Health Foundation approached the Mountrail County Commission with a $25 million request and received $15 million last year and $10 million this year.
A construction crew with McGough works Feb. 24 inside a new long-term care facility that is coming to fruition in Stanley.
“I thank them and credit them for that donation, for allowing this project to happen,” Everett said. “I cannot thank the county enough for their support and having the vision of wanting to support their local nursing home and see it survive.”
The $25 million will pay the bulk of the nursing home construction cost. As of February, the foundation had $14 million yet to raise through donations and grants to fully fund the $53 million project.
Eight local Lutheran churches that have ownership in Mountrail Bethel Home also are looking at ways to support the project. Community financial support is critical to be able to make the improvements, Everett said.
“You don’t make money running a nonprofit, rural nursing home or rural hospital,” she said. “You literally are doing it for your community. You want to bring in the best providers. We’re blessed to have local providers.”
A future phase of the proposed construction includes a new hospital gift shop, extended ambulance bay and extended hospital waiting room.
Equipment and crews with McGough break up ground where work is ongoing on Mountrail County Health Center’s new long-term care facility Feb. 24.
This spring, construction will start on the ambulance garage. That work is set for an October completion. The waiting room in the middle of the hospital will move closer to the ambulance side of the building.
The kitchen will double in size during renovation scheduled to commence in March 2026 and finish in 2027. Additionally, the 11-bed, critical access hospital, built in 2001, will get a new entrance.
Once the new nursing home opens, both the north and south wings of the existing facility will be demolished, allowing expansion of the hospital and creation of a parking lot. A single parking lot ending in a circular driveway in front of the facility will connect the access points to the nursing home, hospital and clinic.
The hospital expansion will include space for MRI equipment and an infusion suite, both of which will be new offerings that will allow for more outpatient services, Everett said. Pharmacy will be getting a new suite, and a suite area will be created for outside specialists who come to provide care.
“We have six specialists that come in now, but we need to designate a space for it because it’s just getting too tight in the clinic,” Everett said.
The expansion construction is scheduled for July 2026-September 2027.
Rosen Place on 8th Assisted Living and a chapel, both built in 2019, will stay, and a new wing will be added to Rosen Place during 2027. As of February, Rosen Place had a waiting list of 31 individuals. The plan is to add seven more units to the current 14.
If all goes as planned, MCHC will have its new look fully completed by December 2027.
The latest projects come after an earlier series of projects that started about 15 years ago with the addition of a CT scanner, expansion of the emergency room and enclosure for the ambulance bay. That was followed by a clinic expansion and construction of Rosen Place, an executive conference room and chapel.
Stanley, ND — The Leona M. and Harry B. Helmsley Charitable Trust has granted $238,556.00 to Mountrail County Medical Center to purchase a Mindray TE X ultrasound system for the ER and a GE Logiq E10s for the Radiology Department as part of a $27.4 million ultrasound initiative in North Dakota.
The initiative includes more than $21.8 million to help 69 North Dakota hospitals and health centers purchase ultrasound imaging devices and nearly $5.7 million to boost sonography and point of care ultrasound (POCUS) training opportunities across the state.
“The Helmsley Foundation has provided the ability for our radiology department to bring more advanced ultrasound services to Mountrail County and our neighboring communities”, explains Brenna Williams, Radiology Manager for MCMC. “Our new machine will provide higher quality echocardiograms and more detailed imaging in pre-natal and breast exams along with general, vascular, and pediatric ultrasonography. The generosity of the Helmsley Foundation will play a key role in achieving superior diagnostic imaging and setting the standard for exceptional rural health care. Ultrasound uses high-frequency sound waves to produce images of structures inside the body. This safe, cost-effective tool supports other clinical information to help providers make timely diagnoses and provide appropriate treatment.”
Walter Panzirer, a Trustee of the Helmsley Charitable Trust, said the grants will help improve access to top-notch medical treatment for North Dakotans, whether they live in Fargo, Bismarck, or Grand Forks, or a smaller rural community such as Bottineau, Rugby, or Hettinger.
“These grants will help ensure that hospitals and health centers across North Dakota have the latest in state-of-the-art ultrasound equipment and training,” Panzirer said. “Facilities need to stay current with rapidly advancing technology so they can continue to provide the very best healthcare close to home.”
The majority (134) of the devices purchased through the grants are POCUS machines, which are used by providers at the bed or tableside for immediate assessment of a patient to quickly determine a course of action. The grants will also provide 57 general ultrasound systems and 24 cardiovascular ultrasound systems, which aid in imaging of the heart.
“The Helmsley grant has allowed us the ability to update our point of care ultrasound system to provide further advanced technology to the Mountrail County Medical Center bedside,” states Brittany Haugtvedt, MCMC’s ER DON. “The new ultrasound system offers a full suite of innovative features and AI powered Smart Tools to help expedite clinical decision making. We are very grateful to the Helmsley Foundation for allowing us to have the best-in-class imaging to help provide a higher standard of care in the rural health care setting.”
The initiative also includes nearly $1.9 million to North Dakota State University and nearly $3.8 million to High Quality Medical Education (HQMEDED) to expand sonographer expertise and provide comprehensive POCUS training to doctors, physician assistants, and nurse practitioners. Additionally, more than $64,000 will go to individual facilities to boost sonographer training.
The Helmsley Charitable Trust has committed a total of $72 million to fund ultrasound equipment and training initiatives for rural communities and underserved populations in Nevada, North Dakota, Minnesota, and Wyoming.
The Leona M. and Harry B. Helmsley Charitable Trust aspires to improve lives by supporting exceptional efforts in the U.S. and around the world in health and select place-based initiatives. Since beginning active grantmaking in 2008, Helmsley has committed more than $4.5 billion for a wide range of charitable purposes. Helmsley’s Rural Healthcare Program funds innovative projects that use information technologies to connect rural patients to emergency medical care, bring the latest medical therapies to patients in remote areas, and provide state-of-the-art training for rural hospitals and EMS personnel. To date, this program has awarded more than $750 million to organizations and initiatives in the states of Hawaii, Iowa, Minnesota, Montana, Nebraska, Nevada, North Dakota, South Dakota, Wyoming, and two U.S. Pacific territories, American Samoa and the Commonwealth of the Northern Mariana Islands. For more information, visit www.helmsleytrust.org.
Each January, we recognize Cervical Health Awareness Month to help raise awareness around cervical cancer. January may be coming to a close, but there’s never a bad time to talk about cancer prevention!
The American Cancer Society estimates there will be 13,360 new cervical cancer diagnoses in 2025, along with 4,320 deaths. But thankfully, cervical cancer is preventable and highly treatable if caught early via regular screenings.
In this blog, we’ll explore what you should know about cervical cancer, how to prevent it, and what to expect when you schedule a screening.
What You Need To Know About Cervical Cancer
Cervical cancer develops in the cervix, the lower part of the uterus that opens into the vagina. Almost all cases of cervical cancer are caused by the human papillomavirus, or HPV. HPV is extremely common and can be spread through skin-to-skin contact.
Most of the time, HPV infections are cleared by the immune system without causing symptoms. But in some cases, an HPV infection can lead to cervical cancer, which can take anywhere from 5-20 years to develop.
In its early stages, cervical cancer often presents no symptoms. However, if you experience the following, it’s important to consult with your doctor right away, as they could be symptoms of cancer in your cervix:
Irregular bleeding between periods, after menopause, or after sexual intercourse
Increased or foul-smelling vaginal discharge
Persistent pain in your back, legs, or pelvis
Weight loss, fatigue, and loss of appetite
Vaginal discomfort
Swelling of legs
With early diagnosis and effective management, cervical cancer is a highly treatable form of cancer. But successful treatment relies on early detection.
Cervical Cancer Prevention
Cervical cancer is a highly preventable and treatable form of cancer, so regular screenings are important.
There are two common types of screening tests: the HPV test and the Pap test or “Pap smear.” The first tests for the HPV virus itself, and the second tests for precancerous cells on the cervix that might become cancer if they aren’t treated.
The U.S. Preventive Services Task Force (USPSTF) recommends women start getting Pap tests every three years beginning at age 21. From 30 to 65 years of age, they recommend: the Pap test alone every three years; a high-risk HPV test alone every five years; or “co-testing” for both every five years. Testing isn’t recommended for most women over 65.
What To Expect in Your Cervical Cancer Screening
Both of these screening tests are available through your doctor’s office or clinic. Talk with your primary care physician about what your testing schedule should be.
When you go in for your Pap test or HPV test, your doctor or gynecologist will use an instrument called a speculum to examine your vagina and cervix. During this examination, they will collect a few cells and mucus from the cervix and the surrounding area.
These cells will then be sent to the lab for testing. For a Pap test, the cells will be examined for abnormalities. For an HPV test, the cells will be tested for HPV. It may take several days or even a few weeks to receive your test results.
If your test results are normal, that means there is very little chance you will develop cervical cancer in the next few years, and your doctor will most likely recommend regular screenings every three to five years.
If your test shows abnormal cells, your doctor will contact you with next steps. Keep in mind that even if your test results are not normal, that doesn’t necessarily mean you have cancer—there are many reasons test results could show abnormalities. It’s important to follow up with your doctor right away to discuss your results and determine what, if any, treatment is necessary.
If it’s been a while since you had a Pap test, consider this Cervical Health Awareness Month your reminder to schedule one! Contact the clinic at 701-628-2505 today to schedule your next visit.
Created in 2011 by the National Organization of State Offices of Rural Health (NOSORH), National Rural Health Day is an annual celebration of rural healthcare providers and other organizations dedicated to addressing the unique healthcare needs of rural communities.
With dozens of webinars and other events highlighting various aspects of rural healthcare, National Rural Health Day helps healthcare providers, community partners, and individuals celebrate the healthcare wins and address the struggles of their communities.
This year’s National Rural Health Day was on Thursday, November 21st. To celebrate at MCHC, we asked some of our long-term staff what they think is the power of rural healthcare. Here’s what they had to say.
An Interview With MCHC Staff: The Power of Rural Healthcare
Jim Clark—Director of Plant & Maintenance, 37 Years of Experience
What do you love about working in rural healthcare?
I love working in rural healthcare because I love providing for a community that I have been part of for most of my life.
What would you say to a college graduate about why they should consider working in rural instead of urban healthcare?
I would ask them if they like living in a small community and getting to know the people they work with. There is more of a personal touch in the small communities.
What do you think is the biggest challenge facing rural healthcare today?
The biggest challenge facing rural healthcare is staffing shortages, as well as finding quality employees.
What traits does someone need to have to work in rural healthcare?
You have to be willing to step up and be able to work in many different departments and wear many different hats.
Pat Aho—Dietary Services, 34 Years of Service
What do you love about working in rural healthcare?
It gives me the chance to help people when they are in the most vulnerable time of their life.
What would you say to a college graduate about why they should consider working in rural instead of urban healthcare?
You have a chance to get to know the people you work with versus in urban healthcare you see so many people, you don’t get the same closeness.
What do you think is the biggest challenge facing rural healthcare today?
I think smaller communities have a harder time keeping up with the benefits they can offer compared to urban areas. Urban areas have more resources and can offer employees more pay and better benefits.
What traits does someone need to have to work in rural healthcare?
I think someone in rural healthcare needs to be compassionate and understanding of people’s wants and needs.
LaDonna Kinnoin—Purchasing/CSR, 35 Years of Experience
What do you love about working in rural healthcare?
I love taking care of people and being able to provide what they need so they do not have to travel so far to get the care they need.
What would you say to a college graduate about why they should consider working in rural instead of urban healthcare?
I would tell them that it is very rewarding.
What do you think is the biggest challenge facing rural healthcare today?
In my job, it’s the cost of supplies. Because we are a smaller facility, we do not get some of the discounts offered when you buy in bulk.
What traits does someone need to have to work in rural healthcare?
Someone working in rural healthcare needs to be friendly, kind, and want to help others.
Janel Borud, RN—Clinic Director, 27 Years of Experience
What do you love about working in rural healthcare?
I love working in rural healthcare because I get to know our patients more intimately due to our smaller population. I have assisted in caring for the same patients from birth to adulthood and cared for their parents and grandparents. It is a sense of community.
What would you say to a college graduate about why they should consider working in rural instead of urban healthcare?
There are plenty of loan repayment/forgiveness options when working in a rural area. Also, due to the deficit of healthcare workers in rural areas, facilities work hard to incentivize those open positions. Help in relocating may also be part of the incentive package. Being rural also means specialists are few and far between, giving you the opportunity to see a wider scope of patients and gaining a great deal of experience.
What do you think is the biggest challenge facing rural healthcare today?
Lack of healthcare workers, increased cost of delivering care, insurance companies not paying enough for the cost of care for patients, and the inability of the patients to pay their share of the high treatment cost. I don’t think this is only an issue within rural healthcare, as healthcare facilities in urban areas are seeing this as well.
What traits does someone need to have to work in rural healthcare?
They need to enjoy a slower pace of life, be adaptable and versatile, enjoy community, and have a team player mentality.
Taina Karow, RN — 39 years of experience
What do you love about working in rural healthcare?
I love rural healthcare because it is extremely rewarding to me to do what I love in such a wonderful community of people who I have come to know and love, with genuine concern for their wellbeing.
What would you say to a college graduate about why they should consider working in rural instead of urban healthcare?
It is the heartfelt care I want to give our patients, always knowing that I am caring for someone’s loved one as I would my own. This comes easily because of the interpersonal relationships that develop in a rural community.
I am also thankful and honored to work in a rural hospital, as a team player who cares about others and works together for the common good of our patients. Each day we have an opportunity to make a difference in someone’s life. That is the beauty of community and rural health. For the small things I do, it comes back to me tenfold.
Please join us in thanking the entire MCHC team for their dedicated work throughout the year to ensure our community has the quality healthcare they need to thrive. Together, we’ll continue to build a healthy community for many years to come.
Looking for a career in rural healthcare? MCHC is hiring! Check out our careers page for open positions.
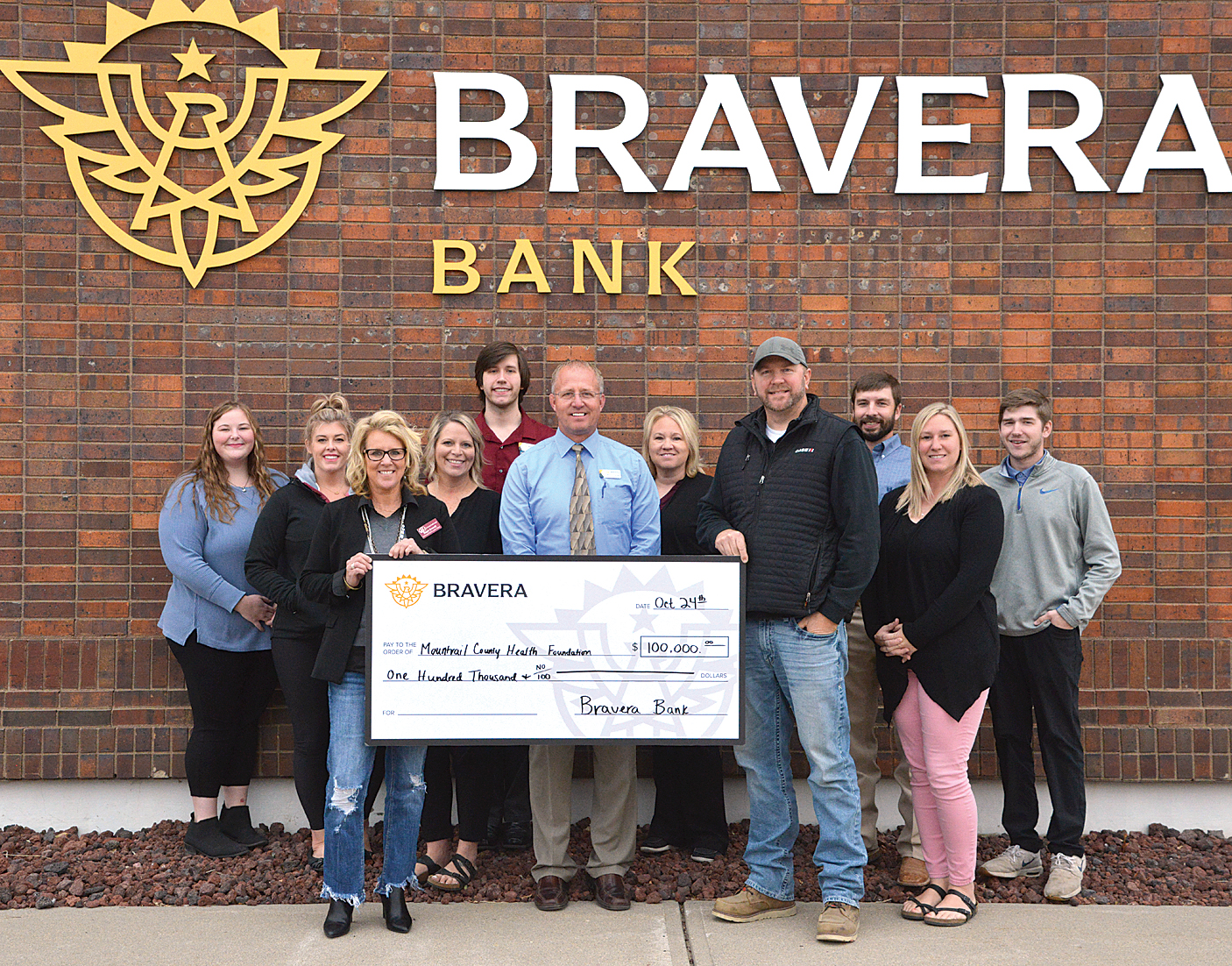
Bravera Bank: A Longtime Supporter of MCHC and the Surrounding Community
Stanley branch Market President Heath Hetzel says that Bravera focuses on giving back and supporting their communities. The hospital and nursing home are a huge part of not just Stanley, but all surrounding communities.
When Bravera sees a need across their footprint, they want to support and be a part of meeting that need. Youth and healthcare make up a large part of where they want to allocate their giving, as hospitals and schools are two of the largest employers within communities.
Our own Steph Everett, Administrator of Mountrail Bethel Home and CEO of MCMC shared:
“Bravera Bank has been a longtime supporter of the building projects at the Mountrail County Health Center over the years. We are thankful for their ongoing leadership and support in improving our community, and are so grateful for their generosity and what a blessing they are to the new Nursing Home project.”
MCHC Building Project Timeline
The first phase of construction for the MCHC project is our new 36-bed nursing home (including ten basic care rooms), the same number of beds as the current nursing home. This Nursing Home phase is expected to take roughly two years and, once completed, will come up to where the current north wing is located.
On the hospital side, renovations will start with a new entrance near the existing sunroom at Mountrail Bethel Home (MBH). There will be a gift shop and a new waiting room. Construction down the current south wing of the nursing home will include adding an out-patient infusion suite, a pharmacy suite, and an MRI suite.
In addition, purchasing will be moving from the basement to the upper level. The downstairs area will be renovated to accommodate a new specialty clinic that will allow us to bring in more specialists and include a minor procedure room. The ambulance bay by the emergency room will be extended to accommodate the larger sizes of newer ambulances.
As the final part of construction, we will also be adding seven new single apartments to Rosen Place. The assisted living facility currently has a waiting list of 31, showing the need for the new apartments. These apartments will be located along the rest of the current south wing of the nursing home.
Thank you, Bravera Bank, for your generous donation!
With work slated to begin on the new MCMC project this summer, a farewell to Centennial Court was held on Wednesday, May 29. The public was invited to the event that included a short program and a time to share memories of Centennial Court.
Pastor Erin Tormanen opened the program by quoting Psalm 71:9, which reads “Do not cast me away when I am old; do not forsake me when my strength is gone,” (New International Version). He said that people are often troubled by the past, present, and future, perplexed by the challenges, but that can be alleviated by placing faith in God’s faithfulness and covenants.
As you look across cultures, all too often those can feel cast off. In his five years in Stanley, he said, he has had the opportunity to share both at the chapel at Bethel Home and Centennial Court and is thankful and give praise for this place that does not cast off, but rather provides a place to come and have a rich life. He also pointed out, it was not the building, but rather the residents and staff that provided the legacy. As the work at Centennial Court comes to an end, God is not done but rather following his plan and what replaces Centennial Court will build a new legacy. Indeed, he said, it is time to yield to the changes, glorify what is to come and rejoice in what has been, as he offered a prayer of blessing.
Ardis Loock, who was the director at Centennial Court for 21 years, shared her memories of what a wonderful place this was to work. While she shared that she hates to see it go, she knows that what will come will be just as nice.
MBH Activities Director Chuck Repnow shared his thankfulness for the location and opportunities it has given for the residents over the years, saying that the community has shown its desire to take care of its loved ones here, providing a quality of life and more. He praised the foresight to provide the connection between assisted living, the nursing home, hospital and aquatic center.
MBH Social Worker Kelly Wilhelmi spoke about the use of the building during COVID, to provide a unit with the staff to take care of them allowing them to stay at home. She said they were able to have their own employees provide care during the worst possible times while also allowing families to be able to visit their loved ones, often times through the windows, but also in the comfort of their own community.
Melissa Peterson, who has worked at Centennial Court since its opening, says that the importance of the facility was the people she got to meet, who she says enriched her life even more than she gave them.
Others attending shared memories of the gathering space, which was used for birthdays, family gatherings and more. Those memories will always be there as the facility moves forward with the new construction.
It has been more than a year since the Mountrail County Health Foundation began the Partnering for the Future Campaign to add new services to the hospital, expand residences at Rosen Place and build a brand new, state-of-the-art nursing home facility. The first phase of the construction will be a new 36 bed nursing home, which will start with the demolition of Centennial Court in July. Once that phase is complete work can begin to remove the old nursing home and begin hospital renovations and finally the addition of new apartments to Rosen Place.
Early detection through routine mammograms dramatically improves your chances of survival. In fact, according to the American Cancer Society, when breast cancer is detected early and is localized to the breast, the 5-year relative survival rate is 99%!
Janis Thompson found this to be true in her own experience. Diagnosed in 2021, within months Janis received chemotherapy and underwent a mastectomy of her right breast. Today, she is a breast cancer survivor — totally cancer-free!
We recently sat down with Janis to hear her story of diagnosis and treatment, as well as her advice for other women who are diagnosed with breast cancer.
When were you diagnosed, and what was your prognosis at the time?
They found something in my right breast in January or February of 2021, and I started chemo in April of 2021. I had my surgery (a mastectomy to remove my right breast) in July — I remember that because it was right after my granddaughter got married.
Luckily, my cancer was localized. When they did surgery, they didn’t find anything in my lymph nodes or anywhere else, so that was good.
How was your breast cancer detected?
I have a mammogram every year. I came over here to Stanley to have it done, and they saw something, so they sent me to Bismarck for treatment. Before the diagnosis, I didn’t have any symptoms, and the only history of cancer in my family was prostate cancer in my dad and brother.
How old were you when you started getting regular mammograms?
I don’t remember exactly, but I was pretty young.
In 1970, when I was 28, they found something in my left breast. I was three months’ pregnant with my son at the time, and the doctor told me that when I went in for surgery, if they found cancer, they were going to have to take both of my breasts and my baby. So it really scared me. But, thankfully, everything turned out to be fine.
After that, I had to go to the doctor a lot because they would find these little cysts that they would take out with a syringe. What they removed was always coffee-colored, so they told me it was nothing to worry about.
Where did you receive your treatments?
I was in California at the time of my first surgery in 1970. I moved back home to North Dakota in 1972, so my treatments after that were done here. My surgery and chemo treatments were done at Sanford in Bismarck, and I received my other care at MCHC in Stanley.
What was your experience like there?
It was wonderful, he was a great doctor (Dr. Bennett at MCHC). This is crazy, but I felt so close to him — he knew everything about my breasts!
When I was diagnosed in 2021, I had chemo first, and I was kind of sick from it. I gained weight because I didn’t feel well and couldn’t do as much as I usually would.
The type of cancer I had was called spindle cell neoplasm. My oncologist (Thandiwe Gray, M.D.) told me there were five of us who had the same kind of cancer at the same time, and we had the same chemo (which was different from other kinds of chemo).
My chemo was from April to July of 2021, and my surgery was in July of 2021. By December, I was starting to feel like myself again. I went in for a lung biopsy between my surgery and then, because they thought I had lung cancer (but it turned out to be nothing). When we went in for the diagnosis, I cried because I was so happy!
Now, I’m following up with yearly mammograms.
Any advice you’d share with other women going through breast cancer treatment right now?
Have a support system, that’s the main thing. My husband was so good! My daughter and granddaughter did a lot for us too. They came over and did things for us. My granddaughter brought us groceries, and they both came and cleaned the house. At the time I was scared I’d go out and get COVID too, you know, so the only place we went was to the clinic in Bismarck.
I had company at that time, and they didn’t want to get me sick, because you’re so susceptible to disease. So when people came to visit us, they’d visit in the garage or outside when it was warmer. It was hard.
Even now, you have to stay away from people for a while after chemo, because of all the stuff you could get. Don’t think you can run around as much as you did before! You have to take care of yourself.
After a while, though, you have to get out and do stuff — don’t let yourself get stuck inside for too long! I was stuck inside for a year or more, scared to go out. I started back volunteering at the nursing home a couple of months ago now. I worked there for years. Now I go on Friday nights and dance with them.
I’m doing great now. Well, I have other things — I have to have knee surgery in June, and I had my right shoulder done about 5 months ago…all kinds of operations! The scariest one was the breast cancer, though, it really was.
Another thing that helped me get through my treatment was that I read from my Bible and from the Jesus Calling devotional (by Sarah Young) every day — it’s something I always do and have done, but I wouldn’t have been able to get through it all without my Jesus.
Early Detection Could Save Your Life. Schedule Your Mammogram Today!
Thank you, Janis, for sharing your story with us! And congratulations on being cancer-free!
Take a page out of this breast cancer survivor’s book, and make sure to get routine mammograms — even if you don’t have a family history of cancer. Mammograms are quick, easy, and one of the best things you can do to take charge of your health and invest in your future.
Contact us today to set up your yearly mammogram at MCHC!
March was Colorectal Cancer Awareness Month, but it’s always a good time to schedule your screening!
Since 2000, March has been the time for colon cancer patients, survivors, caregivers, and advocates join together to spread awareness of colorectal cancer and the importance of prevention.
In honor of this year’s Colorectal Cancer Awareness Month, we sat down with Abbey Ruland, PA-C at Mountrail County Medical Center, to learn her best tips and helpful information about colorectal cancer screenings. While Colorectal Cancer Awareness Month has passed, these things are always important to keep in mind.
Read on to learn some facts about colon cancer, the recommended timeline for screenings, and the different types of screenings available.
Did You Know…? Facts About Colon Cancer
Each year, around 150,000 people are diagnosed with colon cancer in the U.S.
It is the fourth most commonly diagnosed cancer and the second deadliest type of cancer in the U.S. The average age of diagnosis is 66 years old, but people in their 40s and 50s are increasingly being diagnosed as well. In fact, about 10% of those diagnosed with colorectal cancer are now under age 50.
The good news is that screenings can detect colorectal cancer — and when detected early, it is a highly treatable form of cancer. While more than 50,000 people will die from colon cancer this year, many more will survive their diagnosis, thanks to regular screenings.
How Often Should You Have a Colorectal Cancer Screening?
Previously, it was recommended that people start to get regular colon cancer screenings once they hit age 50. However, due to the increasing trend of colon cancer in younger people, that recommendation has changed — we now recommend screening starting at age 45.
If caught in the early (precancerous) stages, colon cancer or colonic polyps can easily be removed during a colonoscopy. This is great news, because that means those polyps cannot continue to grow into colon cancer! In fact, if everyone had their screening done early enough, we could nearly wipe out advanced colon cancer.
But having a colonoscopy is not exactly everyone’s idea of fun (it would be strange if it was!), so let’s talk about the various screening options available.
What Colon Cancer Screening Options Are Available?
Colonoscopy
The “gold standard” in colon cancer screening is the colonoscopy. This procedure is done at an outside facility: Most of our patients have them done in Minot, Tioga, or Bismarck, but we are happy to arrange your screening where it is most convenient for you.
A colonoscopy usually involves a day of “prep” in which the colon is cleaned out. This involves drinking clear liquids, taking laxatives, and spending a significant amount of time in the bathroom. Then the next day, you go to the facility for the colonoscopy, are sedated, and a surgeon uses a camera to look through the colon to find any abnormalities. (Note that because you are given sedation for the procedure, you will need to have a driver pick you up afterwards.)
The best part of a colonoscopy is that if any polyps are found, they can be removed, and the problem is solved before it even begins!
If your colonoscopy is totally normal, we recommend having one every 10 years.
DNA Stool Testing and FIT Tests
For many patients, a colonoscopy is not the only screening option available. There are a number of less invasive screening tools, including DNA stool-based testing (a.k.a., Cologuard) and FIT tests.
To qualify for either of these tests, patients need to be considered “low risk.” This means they need to have no family history of either colon cancer or precancerous polyps. Also, patients who have a history of precancerous polyps on previous colonoscopies do not qualify for stool screening tests.
DNA stool testing consists of a kit you can receive in the mail. You then place a stool sample in the appropriate container and mail it back to the company. The company will test the stool for blood and other DNA markers that can indicate colon cancer or precancerous polyps.
If your results are negative, we recommend retesting every three years. If your results are positive, that may mean the test found cancer, but more commonly it means it found precancerous polyps that need to be removed. We would then schedule you for a colonoscopy for further evaluation, and if there is a precancerous polyp it will be removed during the procedure.
The FIT test is more basic than the DNA test, as it only checks for blood in the stool. This test needs to be completed yearly and is a little more likely to miss a cancer or precancerous polyp. Again, if the test returns a positive result it would be followed by a colonoscopy for further evaluation.
Neither of these tests require any prep, and both can be done from home, keeping you from missing a day or two of work.
In addition, we now have standing orders in place for our patients for these tests, which means if you’re a regular patient who is at low risk, you can give us a call, speak to a nurse, and place an order for these tests to be completed…without even coming in for an appointment!
Schedule Your Colorectal Cancer Screening With MCMC Today
At MCMC, our goal is to help each of our patients live their longest, best life. We want to find problems before they begin — which is why colorectal cancer screening is so important. We encourage you to schedule an annual wellness exam to make sure we are keeping you in tip-top shape! Please don’t hesitate to schedule an appointment or reach out to the nurses to ask about getting your colorectal cancer screening scheduled today.